Tesamorelin vs Sermorelin: Which Growth Hormone Peptide Is Right for You?
You've done the research. You know your growth hormone levels decline with age — research suggests output can drop by more than half between your 20s and your 60s. You've seen the data on peptide therapy. Now you're looking at two growth hormone releasing hormone (GHRH) peptides — tesamorelin and sermorelin — and trying to figure out which one actually makes sense for you.
Here's what most comparison articles won't tell you: these aren't two versions of the same thing. They share a mechanism — both are growth hormone-releasing hormone (GHRH) analogs that stimulate your pituitary gland to produce more of its own GH — but the intensity, clinical profile, and ideal use case for each are meaningfully different.
Tesamorelin is the higher-intensity option with powerful clinical data behind visceral fat reduction. Sermorelin is the gentler, broader-benefit option that works well for general GH optimization. Neither is objectively "better." The right choice depends on your goals, your body, and what you're trying to accomplish.
This guide breaks down the real differences so you can have an informed conversation with your doctor — not just pick whichever one had the better marketing.
Want to skip straight to finding the right fit for you? Take our 5-minute assessment and a licensed physician will review your profile and recommend the right protocol based on your health data and goals. No appointment needed. Start your assessment ->
What They Actually Are: GHRH Analogs, Not Synthetic HGH
Before comparing tesamorelin vs sermorelin, let's be clear about what you're considering. Neither is synthetic human growth hormone (HGH). Both are growth hormone-releasing hormone (GHRH) analogs — peptides that signal your pituitary gland to produce and release your own growth hormone.
This distinction matters. Synthetic HGH introduces exogenous hormone directly into your system, bypassing your body's regulatory mechanisms. That's why it carries risks like insulin resistance, joint pain, and soft tissue overgrowth. GHRH analogs like tesamorelin and sermorelin work through your body's existing feedback loops — stimulating natural GH pulses rather than overriding them.
Think of it like this: synthetic HGH floods the system with a constant, unregulated dose. GHRH analogs prompt your pituitary to do what it already knows how to do — just more effectively. Your body's negative feedback mechanisms remain engaged, reducing the risk of the runaway GH elevations associated with exogenous GH
If you're familiar with how Enclomiphene works for testosterone — stimulating natural production rather than replacing it — GHRH analogs follow the same philosophy for growth hormone.
Both peptides ultimately drive the same downstream process: your pituitary releases GH in natural pulses, GH travels to your liver and triggers the production of IGF-1 (insulin-like growth factor), and IGF-1 drives the majority of the benefits — fat metabolism, tissue repair, sleep quality, skin and hair improvements, and more. The difference is in how intensely each peptide stimulates that process.
Tesamorelin: The High-Intensity Option
Tesamorelin is a 44-amino acid synthetic analog of GHRH — the full-length molecule with a trans-3-hexenoic acid modification that makes it more stable and resistant to enzymatic breakdown (specifically DPP-4 resistant). This structural advantage gives tesamorelin a longer duration of action and a more potent GH response.
The clinical data is substantial. Tesamorelin earned FDA approval in 2010 (branded as Egrifta) for reducing visceral adipose tissue in HIV patients with lipodystrophy. The pivotal trials demonstrated:
Between 50-100% mean IGF-1 increase — a substantially more powerful GH response than traditional peptides
15% reduction in visceral adipose tissue over 26 weeks, measured by CT scan
Improvements in triglycerides and metabolic markers associated with visceral fat reduction
The word to remember here is intensity. The FDA study showed an 84% IGF-1 increase – significantly more powerful than sermorelin's gentler stimulation. That intensity is what drives the dramatic visceral fat reduction data. It's also what makes tesamorelin the better fit for specific goals.
Where tesamorelin excels
Visceral fat loss: The clinical evidence for targeted reduction of dangerous abdominal fat (the kind wrapped around your organs, not the subcutaneous fat you can pinch) is strong and well-documented.
Body recomposition in already-fit individuals: If you're already exercising and eating well but can't lose the last 5–10 pounds around the midsection, tesamorelin's targeted fat mobilization is designed for exactly this scenario.
Faster, more noticeable results: The higher-intensity GH response generally translates to more visible changes in body composition within the first few months.
What to know
Tesamorelin follows a 5-on/2-off dosing schedule (five days of injections, two days off per week), which helps manage water retention — a more common side effect with the stronger GH response.
The more potent stimulation means side effects like water retention, wrist/hand numbness, and post-injection flushing may be more noticeable than with sermorelin, particularly in the first few weeks.
While FDA approval is specific to HIV-associated lipodystrophy, tesamorelin is prescribed off-label for visceral fat reduction and body composition optimization in broader populations.
Sermorelin: The Gentle, Broad-Benefit Option
Sermorelin is a 29-amino acid analog of GHRH — the biologically active fragment of the full 44-amino acid molecule. It contains everything your body needs to recognize and respond to the GH-release signal, but with a gentler stimulation profile.
Where tesamorelin produces a 50–100% IGF-1 increase, sermorelin delivers a more modest, sustained increase in IGF-1. Enough to meaningfully optimize GH levels while keeping the response moderate and well-tolerated. Sermorelin has decades of clinical use behind it, including previous FDA approval for diagnosing and treating growth hormone deficiency in children, which established a strong safety track record.
Where sermorelin excels
General GH optimization: If your goals span multiple areas — better sleep, faster recovery, improved skin and hair, gradual body composition improvement — sermorelin's broad benefit profile covers all of them without the intensity of tesamorelin.
Sleep quality: GH is released primarily during deep sleep. Sermorelin amplifies this natural pattern, and improved sleep is often the first benefit users notice — frequently within the first 2–4 weeks.
Hair, skin, and nails: Our medical team rates GH peptides 8.5 out of 10 for aesthetic improvements. Nail growth is typically the earliest visible sign (within the first month), followed by improved skin elasticity and hair quality over 3–6 months. Sermorelin's steady, consistent stimulation supports this well.
Recovery: Shorter downtime between workouts, faster tissue repair, less soreness. Users report recovering in one day instead of two between hard training sessions.
First-time peptide users: The gentler response and daily dosing protocol make sermorelin an accessible starting point for anyone new to injectable peptide therapy.
Women: Estrogen upregulates IGF-1, so women tend to get outsized benefit from sermorelin's lower dose — making tesamorelin's higher intensity more aggressive than most women need.
What to know
Sermorelin uses a daily protocol or a 5/2 schedule depending on the dosage amount, typically administered before bed to align with your body's natural nocturnal GH release cycle.
Side effects are generally milder than tesamorelin — some users experience mild water retention, occasional wrist/hand numbness, or post-injection flushing, but these tend to be less pronounced.
Results build gradually. The 3-month minimum protocol applies here — expect sleep improvements first, followed by recovery and aesthetic benefits, with body composition changes becoming noticeable around months 2–3.
Ready to find your match? Take this quiz to find the protocol that fits your goals. Start your assessment ->
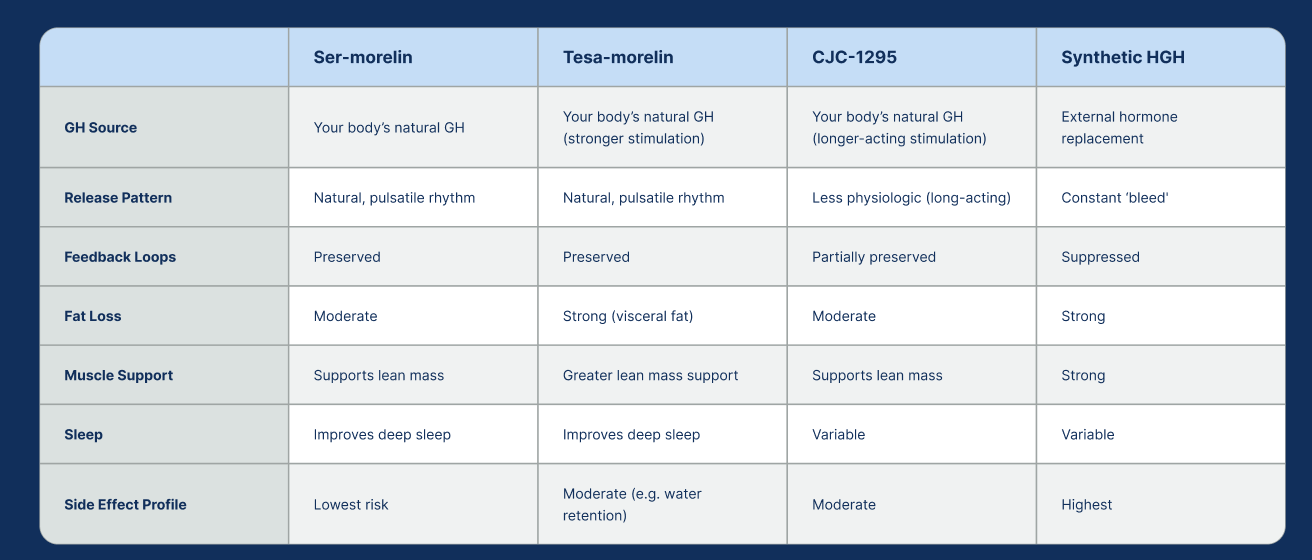
Head-to-Head: Tesamorelin vs Sermorelin
Here's the comparison distilled to what actually matters for your decision:
Need a minimum 3-month commitment before aesthetic benefits appear
Should be injected fasted (at least 1–3 hours after eating, since insulin blunts GH release)
Dosing in the morning before breakfast is also an option (without eating for 30-60 minutes after dosing).
Work synergistically with exercise, proper nutrition, and sleep optimization
Pair well with other protocols like testosterone optimization
Who Should Choose Which
This isn't complicated once you're honest about your primary goal.
Tesamorelin makes more sense if:
Your main goal is losing stubborn belly fat or body recomposition
You're already exercising and eating well but can't move the needle on your midsection
You want the strongest clinical evidence behind your protocol
You're comfortable managing more noticeable side effects in exchange for more aggressive results
You want faster, more visible changes in body composition
Sermorelin makes more sense if:
You're seeking broad GH optimization across multiple areas (sleep, recovery, skin/hair, energy, body comp)
You're new to peptide therapy and want a gentler introduction
You're a woman (estrogen amplifies the IGF-1 response, making the lower intensity more than sufficient)
You prioritize minimal disruption and a mild side effect profile
Your goals are more about sustained vitality and anti-aging than aggressive fat targeting
You want a simple daily protocol without cycling on and off
The honest answer for most people
If you have one specific, measurable goal — losing visceral fat — and the clinical data supporting that outcome matters to you, tesamorelin is the more targeted tool.
If your goals are broader — better sleep, faster recovery, improved skin and hair, gradual body composition improvement, and generally feeling like your GH levels aren't working against you — sermorelin covers more ground with less intensity.
Many people start with sermorelin and consider tesamorelin later if they want to specifically target visceral fat. Others start with tesamorelin for aggressive body recomposition and transition to sermorelin for long-term maintenance. Your doctor can help you determine which sequence makes the most sense based on your labs and goals.
Dosing, Administration, and What to Expect
Both peptides are administered via subcutaneous injection — the same small insulin-type needles used by millions of people daily. Most users describe the injection as virtually painless. It takes about 30 seconds once you're comfortable with the process.
Tesamorelin protocol:
Subcutaneous injection, 5 days on / 2 days off
Inject fasted (at least 1–3 hours after eating)
Dosing in the morning (before breakfast) is also an option, but without eating for 30-60 minutes after dose
Reconstituted from lyophilized powder with bacteriostatic water
Rotate injection sites to prevent irritation
Sermorelin protocol:
Subcutaneous injection, daily
Best administered before bed to align with natural nocturnal GH release
Inject fasted (at least 1–3 hours after eating)
Dosing in the morning (before breakfast) is also an option, but without eating for 30-60 minutes after dose
Reconstituted from lyophilized powder with bacteriostatic water
Upper outer thigh is the preferred injection site
What to expect timeline-wise (both peptides):
Weeks 1–4:
Improved sleep quality is often the first noticeable change. Some users report better energy and mood. Mild side effects (water retention, injection-site reactions) may appear and typically resolve.
Months 1–3:
Nail growth is typically the earliest visible sign of elevated GH. Recovery from workouts noticeably improves. Body composition starts shifting.
Months 3–6:
Measurable changes in body composition, skin elasticity, and hair quality. This is where the protocol really starts to compound. Clinical data on visceral fat reduction (tesamorelin) was measured at 26 weeks.
Monitoring:
Both protocols warrant regular lab work — IGF-1 levels (every 3–6 months), glucose/HbA1c (GH affects insulin sensitivity), and thyroid function. Your prescribing physician will guide the monitoring schedule.
Safety and Side Effects
Both peptides share a common side effect profile, with tesamorelin's typically being more pronounced due to the stronger GH stimulation:
Common side effects (both):
Water retention (more significant with tesamorelin; the 5/2 schedule helps mitigate this)
Wrist or hand numbness (carpal tunnel-like symptoms from fluid retention)
Post-injection flushing
Injection site itchiness or mild irritation (normal — usually resolves with repeated use)
Sleep disturbances (paradoxically, while GH improves sleep long-term, some users experience disruption early on)
Tesamorelin Side Effects:
Clinical trials showed a small percentage of subjects developed impaired glucose tolerance. If you have diabetes risk factors, this needs to be monitored carefully.
Sermorelin Side Effects:
Side effects tend to be milder overall. The primary consideration is individual response variability — some people respond very well, others more modestly.
Contraindications (both):
Active malignancy (GH may promote tumor growth)
Acute critical illness
Hypersensitivity to GHRH analogs
Pregnancy and lactation
Important: These are prescription peptides that require medical supervision. The dosing, monitoring, and protocol adjustments should be managed by a licensed physician — not self-directed based on internet research.
The Bigger Picture: Peptides Are One Piece
Neither tesamorelin nor sermorelin is a standalone solution. The people who see the best results are the ones who treat peptide therapy as an amplifier — not a replacement — for the fundamentals.
What amplifies results:
Consistent resistance training (GH enhances protein synthesis, but you need the training stimulus)
Adequate protein intake (the hormonal environment is only as good as the building materials you provide)
Prioritized sleep (GH is released during deep sleep — poor sleep undermines the entire protocol)
Managed stress (Chronic stress and elevated cortisol blunt the anabolic effects of GH)
What undermines results:
Eating right before injection (insulin blunts GH release — inject fasted)
Inconsistent dosing (both protocols require daily or near-daily commitment)
Expecting results in two weeks (3-month minimum, period)
Ignoring the basics while relying on the peptide to do all the work
Growth hormone peptides work best as part of a comprehensive optimization approach. When combined with proper training, nutrition, sleep, and — where appropriate — complementary protocols like testosterone optimization, the effects compound significantly.
Making Your Decision
The tesamorelin vs sermorelin choice comes down to one question: What's your primary goal?
If the answer is targeted visceral fat reduction and aggressive body recomposition — and you're comfortable with a higher-intensity protocol — tesamorelin is the more precise tool for that job.
If the answer is broader optimization — better sleep, faster recovery, improved skin and hair, sustained energy, and gradual body composition improvement — sermorelin delivers across all of those domains with a gentler approach.
Both are legitimate, clinically-backed approaches to enhancing your body's natural growth hormone production. Both preserve the feedback mechanisms that keep you safe. And both require a real commitment — at least three months of consistent use before you can fairly evaluate results.
The best next step isn't picking a peptide from an article. It's having a conversation with a physician who can review your labs, understand your goals, and recommend the protocol that fits your specific situation.
Ready to find out which GH peptide protocol is right for you?
Start your assessment → it takes about 5 minutes, no appointment needed. A licensed physician will review your profile and help you determine the right approach based on your health data and goals.