Sildenafil vs Tadalafil vs Vardenafil: Which PDE5 Inhibitor Is Right for You?
Most men researching sildenafil vs tadalafil vs vardenafil want a simple answer: which one is best? The honest answer is more useful—and more interesting. These three medications share the same mechanism but create different experiences based on timing, duration, and lifestyle fit. The real question isn't which is objectively superior, but which aligns with how you actually live.
At Maximus, we prescribe all three medications in our Vardenafil, Tadalafil, Sildenafil combination protocol that most providers don't offer. This means we're not invested in pushing one option over another. We're invested in helping you understand what makes each compound distinct so you can optimize for your specific situation—whether that's sexual confidence, gym performance, cognitive function, or all-day vitality.
This guide goes beyond the typical comparison table. You'll get the clinical data that matters, real-world use cases competitors ignore, and a framework for deciding whether one medication fits your life—or whether situational flexibility serves you better. Whether you're a 35-year-old looking to enhance workout recovery, a 50-year-old managing relationship dynamics, or simply curious about what these compounds actually do, you'll leave with a clear understanding of your options.
How PDE5 Inhibitors Work (The Shared Foundation)
Before comparing sildenafil, tadalafil, and vardenafil, you need to understand their shared mechanism. All three belong to a drug class called PDE5 inhibitors (phosphodiesterase type 5 inhibitors). Here's the biology that matters:
When you're sexually aroused, your body releases nitric oxide in penile tissue. This triggers production of cyclic guanosine monophosphate (cGMP), which relaxes smooth muscle cells and allows blood vessels to dilate. More blood flow equals stronger, more sustained erections. Simple enough.
The problem? An enzyme called PDE5 naturally breaks down cGMP, ending the erection. As men age, testosterone levels decline, vascular health deteriorates, and this balance shifts—PDE5 activity can overpower cGMP production. That's where these medications come in. They inhibit PDE5, allowing cGMP to accumulate and blood flow to increase.
Here's what most guides don't tell you: PDE5 isn't only found in penile tissue. It's present in vascular smooth muscle throughout your body—including your skeletal muscles and brain. This is why bodybuilders report enhanced muscle pumps and improved recovery with PDE5 inhibitors (increased blood flow delivers more oxygen and nutrients). Some research suggests cognitive benefits from improved cerebral blood flow, though this application remains off-label.
All three medications—sildenafil (Viagra), tadalafil (Cialis), and vardenafil (Levitra)—achieve the same fundamental outcome: they block the PDE5 response. What makes them different isn't whether they work, but how quickly they start working, how long they last, and how they interact with food and other factors. These pharmacokinetic differences create meaningfully different real-world experiences.
Think of it this way: all three medications turn the same key (PDE5 inhibition), but they open the door at different speeds and hold it open for different durations. Your lifestyle, relationship dynamics, and optimization goals determine which timing profile serves you best.
The Core Differences: Sildenafil vs Tadalafil vs Vardenafil
Here's where sildenafil, tadalafil, and vardenafil actually diverge:
These numbers tell a story about your actual experience.
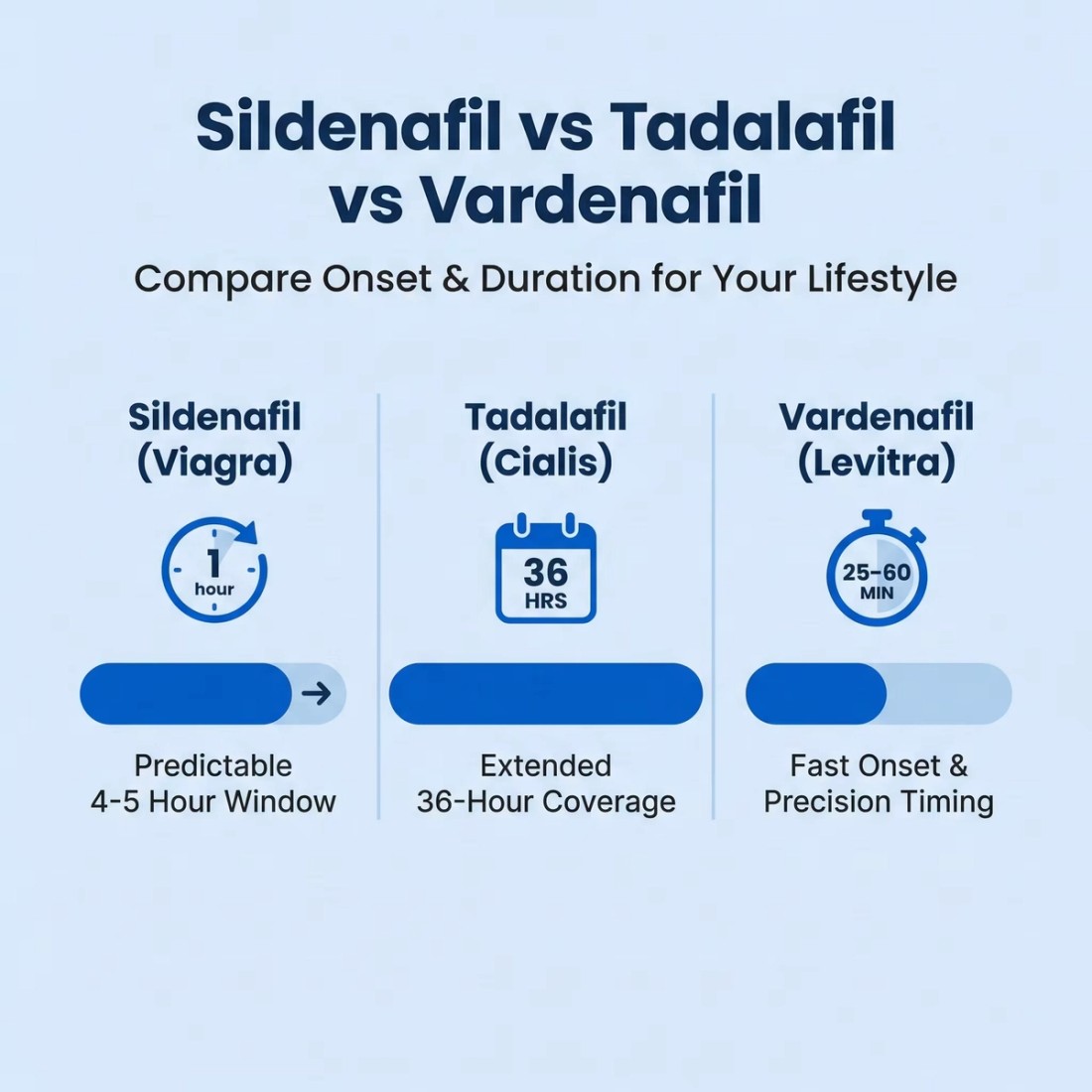
Tadalafil
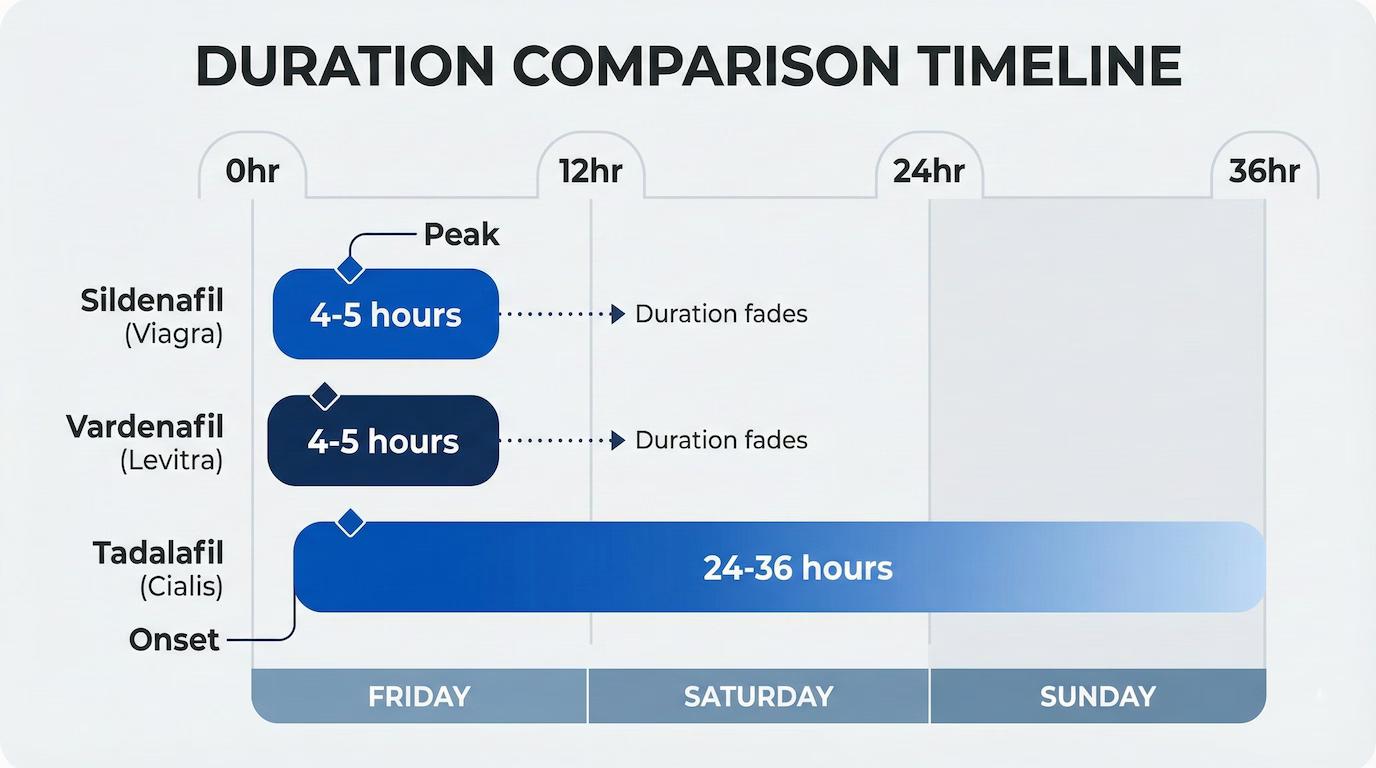
Tadalafil's 36-hour duration means you can take it Friday morning and still have coverage through Sunday—no timing calculations between sessions, no planning around romantic moments. It's often called the "weekend pill" for this reason. The tradeoff? If you experience side effects, they persist longer.
Sildenafil
Sildenafil offers a defined window: predictable 4-5 hour coverage that's long enough for extended intimacy but clears your system by morning. It's been studied the longest (since 1998), so we have the most robust long-term safety data. Some users report a temporary blue tint to vision—rare, but more common with sildenafil than the others.
Vardenafil
Vardenafil is the precision option: slightly faster onset than sildenafil in many users, with similar duration. Clinical trials suggest it may be effective at lower doses for some men, particularly those with diabetes-related vascular challenges. However, food interactions are more pronounced—a heavy dinner can significantly blunt its effectiveness.
Potency comparison: Milligram-for-milligram, vardenafil is roughly 10x more potent than sildenafil, and tadalafil sits between them. But potency doesn't equal effectiveness—it just means you need different doses to achieve the same result. A 10mg tadalafil dose approximates a 50mg sildenafil dose in clinical effect.
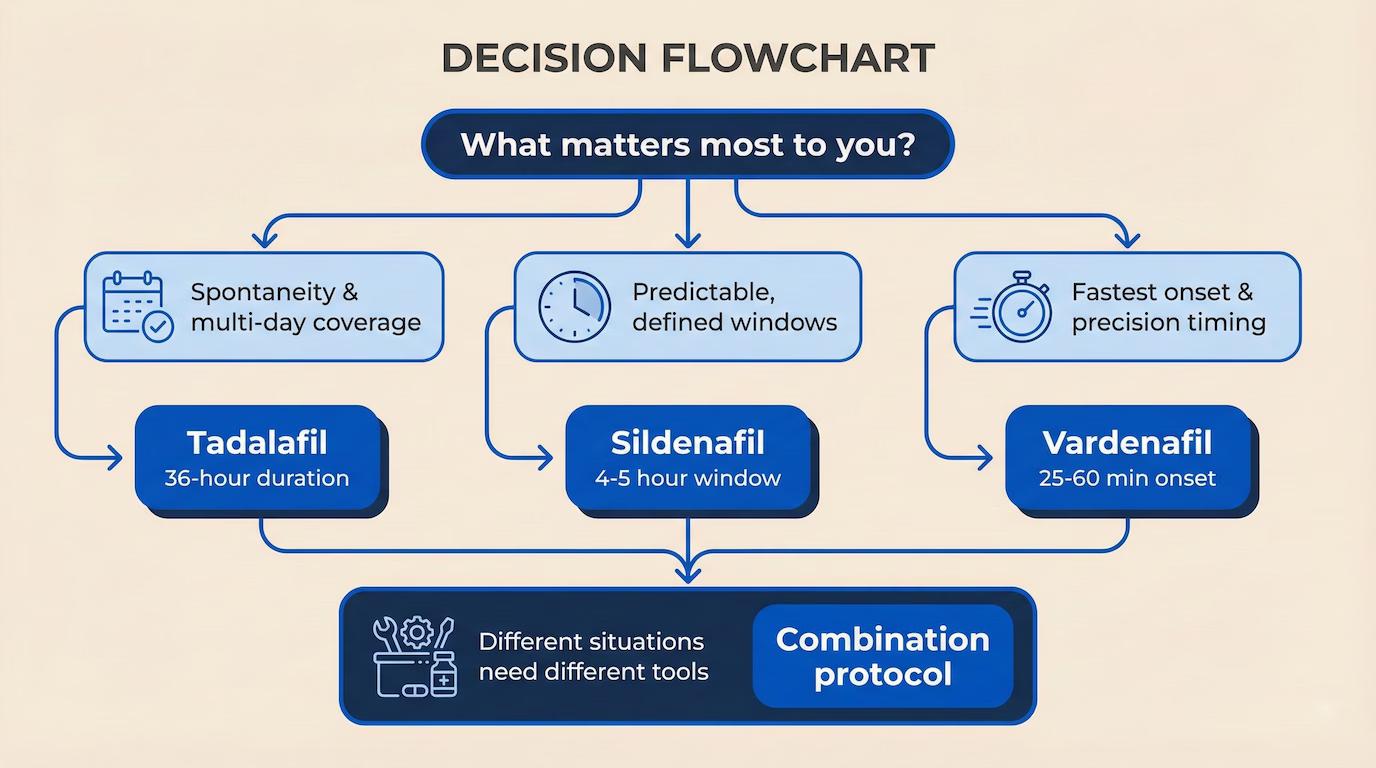
The key insight? There's no universal "best" choice. Your ideal medication depends on whether you prioritize spontaneity (tadalafil), predictability (sildenafil), or rapid onset with precision timing (vardenafil).
Which One Should You Choose? Consider Your Lifestyle and Goals
The right decision depends entirely on your lifestyle patterns and optimization goals.
If your relationship involves spontaneous intimacy—weekends away, unpredictable schedules, multiple sessions across days—tadalafil's 36-hour window eliminates performance anxiety. You're covered without timing calculations. Many Maximus clients in long-term relationships prefer this "set it and forget it" approach. Take it Friday morning, enjoy the entire weekend without pharmaceutical logistics.
If you prefer predictable windows with clear start and end times, sildenafil delivers exactly that. You know when it kicks in (60 minutes), when it peaks (2 hours), and when it clears (5-6 hours). This predictability appeals to men who want precise control or are testing how their body responds. It's also ideal if you're alternating between gym use (see next section) and sexual use—you want the compound out of your system for certain activities.
If you're dealing with diabetes-related ED or want the fastest possible onset, vardenafil often performs best. Studies show superior effectiveness in diabetic populations, and some users report feeling effects in 20-25 minutes. The precision matters when timing is tight or you want to minimize the planning window.
Beyond sexual performance, your broader optimization goals shape the decision. Training for a competitive event or focused on body composition? Tadalafil's extended duration means sustained blood flow benefits across multiple workouts from a single dose. Experimenting with cognitive support during deep work sessions? Some users find tadalafil's long half-life provides all-day cerebral circulation benefits.
Here's what differentiates Maximus's approach: we map your typical week—relationship patterns, training schedule, performance goals—then match you to the medication (or combination) that fits your actual life.
For Sexual Performance Optimization
Let's get specific, because "better erections" oversimplifies what different men actually need.
The new relationship scenario. You're 42, recently divorced, dating someone new. Performance with an unfamiliar partner creates natural uncertainty. Sildenafil offers a defined window of reliable support. Take 50mg about an hour before you expect things to progress. You know you have coverage for the evening, but if the timing shifts, it's out of your system by morning.
The established relationship with variable timing. You're 55, married 20 years. Intimacy happens organically—sometimes mornings, sometimes late nights, occasionally spontaneous afternoons. Tadalafil 10mg on Friday and Monday mornings provides continuous coverage without per-event timing. The logistics disappear.
The refractory period optimizer. You're 38, notice longer recovery times between rounds than you'd like. Vardenafil 10mg 30 minutes before intimacy not only supports initial quality but helps maintain responsiveness for second or third rounds within the 4-hour window.
The pattern: match the medication's duration and predictability to your relationship dynamics and sexual rhythm. Not just "does it work" but "does it work for how you actually have sex."
Workout and Cognitive Applications
For optimization-focused users, here's where sildenafil vs tadalafil vs vardenafil gets interesting. The same mechanism that improves erectile function enhances performance in other domains.
Pre-workout muscle pump and endurance. Bodybuilders and serious lifters have used these compounds off-label for years. Tadalafil 2.5-5mg daily provides continuous PDE5 inhibition, translating to enhanced muscle pumps (increased blood volume in working muscles), improved nutrient delivery, and potentially faster recovery. Research in pulmonary hypertension patients shows improved exercise capacity—similar cardiovascular benefits may apply to healthy athletes. Take it in the morning; it works throughout your training day. For detailed protocols, see our tadalafil pre-workout guide.
High-altitude performance. Planning time at elevation? Tadalafil is prescribed for altitude sickness because improved circulation helps offset low-oxygen environments. Users report better stamina and faster acclimatization at 10,000+ feet.
Cognitive work sessions. Some biohackers experiment with low-dose tadalafil (2.5-5mg) for sustained focus during deep work. The theory: enhanced cerebral blood flow supports cognitive performance. Evidence is anecdotal rather than clinical, but users report subjective improvements in concentration during 4-6 hour creative sessions.
For these applications, tadalafil's extended duration dominates. You want all-day coverage, not a 4-hour window. Sildenafil and vardenafil work for targeted pre-workout use but require precise timing—less practical for spontaneous training.
The Case for Combination Protocols
Here's where we move beyond the standard "pick one" advice—because for many men, the most sophisticated answer isn't choosing a single medication. It's having access to different tools for different situations.
Consider the logic: tadalafil excels at baseline coverage and spontaneity. Sildenafil and vardenafil offer peak intensity in defined windows. These aren't competing options—they're complementary tools.
The baseline + boost approach: Some men take low-dose tadalafil (5mg) daily for consistent blood flow benefits—workout support, spontaneous intimacy coverage, general vascular health. When they want maximum effect for a specific occasion, they can layer sildenafil or vardenafil on top. This provides the extended coverage of tadalafil plus the peak intensity of a shorter-acting compound. Clinical oversight is essential to manage the cardiovascular considerations.
Situational flexibility without daily dosing: Other men prefer keeping all three available and choosing based on the situation. Tadalafil for weekends away. Sildenafil for date nights with predictable timing. Vardenafil when rapid onset matters. This approach requires understanding each medication's profile, but offers genuine adaptability.
The limitation of "pick one" advice: Most telehealth services default to prescribing one medication because it's simpler operationally. But simpler for them doesn't mean optimal for you. If tadalafil's duration is ideal for weekends but you'd prefer a shorter-acting option during the workweek, why should you have to choose?
This is why Maximus offers vardenafil, tadalafil, and sildenafil together—with physician guidance on how to use each strategically. You get the medication that fits each situation rather than forcing one compound to serve every scenario.
Combining with complementary mechanisms: Beyond PDE5 inhibitors, PT-141 (bremelanotide) works through melanocortin receptors rather than vascular pathways. PT-141 increases libido and arousal; PDE5 inhibitors handle the mechanical response. For men experiencing reduced desire alongside erectile challenges, this combination addresses both dimensions—something a single medication can't accomplish.
Safety note: Combining PDE5 inhibitors increases cardiovascular load and side effect potential. This is why physician-guided protocols matter—proper dosing, timing guidance, and monitoring based on your health profile. Forum-based self-experimentation is risky. Clinically designed combinations with medical oversight are optimization tools.
Switching Between Medications: What to Expect
Here's something that stops many men from even starting: fear of committing to the wrong choice. What if sildenafil doesn't feel right? Can you switch to tadalafil? Do you start over?
Let's be clear: switching between sildenafil, tadalafil, and vardenafil is expected, not exceptional. Your first prescription is an educated starting point, not a permanent decision. Individual response varies based on metabolism, vascular health, and factors you can't predict until you actually try.
The washout period matters. Because these medications share a mechanism, you should let one clear before starting another. With sildenafil or vardenafil (4-5 hour half-lives), 24 hours is sufficient. With tadalafil (17.5 hour half-life), wait 48-72 hours before switching. This prevents overlapping cardiovascular effects and lets you assess each medication clearly.
Common switching patterns we see:
Sildenafil to tadalafil:
A man finds sildenafil effective but dislikes coordinating around the 4-hour window. Tadalafil provides similar support with more flexibility. Dosing adjusts accordingly (50mg sildenafil ≈ 10mg tadalafil in clinical effect).
Tadalafil to vardenafil:
Lingering headaches from tadalafil's 36-hour duration become annoying. Vardenafil's shorter action reduces side effect exposure while maintaining effectiveness.
Vardenafil to sildenafil:
Food interactions with vardenafil prove impractical (dinner dates become logistical puzzles). Sildenafil's milder food impact improves real-world usability.
The key difference between transactional prescription services and ongoing optimization: most platforms make switching cumbersome—new questionnaire, new approval process, new fee. It's designed for one-and-done prescribing, not iterative refinement.
At Maximus, finding the right solution or combination is part of the process. Your physician reviews what worked, what didn't, and what you're optimizing for. We adjust medications, doses, and protocols as your needs evolve. This is how optimization actually works—iterative, responsive, personalized.
Cost Considerations: Generic vs Brand
Let's talk pricing—because cost matters and most providers obscure it until checkout.
Generic vs brand: Generic sildenafil, tadalafil, and vardenafil contain the same active ingredients as Viagra, Cialis, and Levitra but cost 80-95% less. Sildenafil went generic in 2017, tadalafil in 2018, vardenafil in 2018. Unless you specifically need brand packaging, generics offer the same base compound at a fraction of the cost. At Maximus, we prescribe generics as standard—no reason to pay brand premiums for identical molecules.
Typical pricing landscape:
Budget pill delivery services: $2-5 per dose for generic sildenafil/tadalafil. Attractive price point, but you're getting medication only—no dosing optimization, no protocol adjustment, no physician guidance beyond initial approval. Reasonable if you already know exactly what works for you.
Traditional pharmacy with insurance: Highly variable. Most insurance doesn't cover ED medications. Out-of-pocket runs $10-50+ per dose depending on pharmacy and coverage, plus the awkwardness of the local pickup.
Optimization-focused services (like Maximus): Medication plus physician consultations, protocol development, combination options, and ongoing support. You're paying for expertise and customization, not just pills.
The value equation most people miss: If you spend $2 per dose on a medication that isn't optimally matched to your physiology, you're paying for subpar results. If you pay more per dose with physician guidance ensuring maximum effectiveness and minimal side effects, you're getting better return on investment. Cost per optimized outcome matters more than cost per pill.
Additionally, combination protocols and advanced options aren't available through budget services. Strategic PDE5 combinations, PT-141, testosterone optimization—these require medical sophistication that pill delivery platforms don't offer.
Maximus pricing includes medication, physician consultations for protocol adjustments, and access to our full range of optimization compounds. You'll pay more than the cheapest option, less than traditional urology practices, and you'll get physician-guided optimization rather than algorithmic prescribing.
Safety Profile: Side Effects and Contraindications
PDE5 inhibitors have been studied extensively for over 25 years. They're remarkably safe for most men when used appropriately. But "most men" isn't all men, and "appropriately" requires understanding contraindications.
Common side effects (affecting 10-30% of users):
Headache: Most frequent complaint across all three. Results from vasodilation in cerebral blood vessels. Usually mild and often decreases with continued use. Hydration and lower doses help.
Flushing: Facial redness from increased blood flow. Temporary and harmless, though socially noticeable for some.
Nasal congestion: PDE5 exists in nasal tissue. Results in stuffy nose for 10-20% of users. Tadalafil seems to cause this slightly more often.
Indigestion: Mild dyspepsia from smooth muscle relaxation in the GI tract. Taking with food reduces this (except vardenafil, where food interferes with absorption).
Rare but serious side effects:
Priapism: Erection lasting >4 hours. Medical emergency requiring immediate treatment. Occurs in <0.1% of users.
Vision changes: Temporary blue-tinted vision or light sensitivity (more common with sildenafil). Rare cases of NAION—sudden vision loss linked to underlying vascular disease.
Hearing changes: Extremely rare sudden hearing issues. Stop medication immediately and seek medical attention.
Absolute contraindications—do NOT use if:
You take nitrates (nitroglycerin, isosorbide) for chest pain. Combining with PDE5 inhibitors causes severe, potentially dangerous drops in blood pressure.
You've had heart attack, stroke, or life-threatening arrhythmia in the past 6 months.
You have uncontrolled blood pressure (>170/110 or <90/50).
You have severe liver impairment.
Relative contraindications—use with caution and medical guidance:
Cardiovascular disease (your physician needs to assess if physical activity is appropriate)
Conditions predisposing to priapism (sickle cell, multiple myeloma, leukemia)
Long-term safety: Studies following users for 10+ years show no increased risk of cardiovascular events, cancer, or organ damage from chronic PDE5 inhibitor use. Daily low-dose tadalafil (2.5-5mg) has been studied extensively and shows excellent long-term safety.
Here's why legitimate medical oversight matters: sketchy online sources skip health screening, don't check contraindications, and provide no follow-up if issues arise. Physician-guided services review cardiovascular health, current medications, and medical history before prescribing—then monitor your response over time. The medication is safe when prescribed appropriately. "Appropriately" requires actual medicine, not just questionnaires.
Frequently Asked Questions
Can I take sildenafil, tadalafil, or vardenafil with alcohol?
Moderate alcohol (1-2 drinks) is generally fine, though alcohol impairs erectile function independently. Heavy drinking increases side effects (headache, dizziness, blood pressure drops) and reduces medication effectiveness. If you're drinking enough to impair judgment, you're probably drinking enough to impair performance regardless of medication.
Do these medications increase desire or just physical response?
PDE5 inhibitors work on the mechanical side—blood flow and erection quality. They don't directly increase desire or arousal. If low libido is your primary concern, investigate testosterone levels and consider PT-141 (which does influence desire). Many men find improved physical confidence indirectly boosts libido by reducing performance anxiety.
Will I build tolerance with regular use?
True pharmacological tolerance to PDE5 inhibitors is rare. Perceived "tolerance" is usually disease progression (worsening vascular health) or psychological factors. If effectiveness decreases, explore underlying causes—testosterone, cardiovascular health, relationship dynamics—rather than simply increasing dose.
Can I cut pills to adjust dosing?
Yes, most PDE5 inhibitor tablets can be split. Sildenafil and vardenafil tablets are often scored for this purpose. Tadalafil can be split but isn't scored—use a pill cutter for accuracy. Some providers (including Maximus) offer multiple dose options that eliminate the need for splitting.
What starting dose should I expect?
Standard starting doses: sildenafil 50mg, tadalafil 10mg, vardenafil 10mg. Many men find lower doses (sildenafil 25mg, tadalafil 5mg) effective, especially when combined with lifestyle optimization—exercise, sleep, stress management. Start at standard dose, then adjust down if results are good but side effects bother you, or up if response is insufficient.
What if none of these medications work for me?
PDE5 inhibitors don't work for everyone, often due to significant vascular damage, neurological factors, or hormonal deficiencies. Next steps include investigating testosterone levels, trying PT-141 (different mechanism), exploring combination protocols, or discussing advanced options with a urologist. Non-response to PDE5 inhibitors warrants thorough evaluation—it may signal underlying cardiovascular concerns worth addressing.
Are there natural alternatives that work comparably?
No supplement matches PDE5 inhibitor effectiveness. L-citrulline, L-arginine, and panax ginseng have mild supportive effects but won't replace pharmaceutical intervention for meaningful challenges. They can complement PDE5 inhibitors as part of comprehensive optimization but aren't substitutes.
Finding Your Optimal Approach
Understanding the differences between sildenafil vs tadalafil vs vardenafil isn't about identifying a "winner"—it's about matching pharmacokinetics to how you actually live.
Choose tadalafil if you want extended coverage, spontaneity, and multi-day flexibility—and don't mind longer side-effect duration if they occur.
Choose sildenafil if you want predictable 4-5 hour windows with the most extensive safety data and clear on/off timing.
Choose vardenafil if you need the fastest possible onset, have diabetes-related considerations, or want precision timing despite food sensitivity.
Consider access to all three if different situations call for different tools—weekends versus weekdays, planned versus spontaneous, peak intensity versus baseline support.
The sophisticated approach involves physician-guided experimentation. Try your initial selection for several uses, assess honestly, and adjust—switch medications, modify doses, or explore combinations. This is iterative optimization, not one-size-fits-all prescribing.
That's where Maximus differs from standard telehealth. We prescribe all three medications, as well as testosterone therapy treatments. We design protocols based on your goals, not algorithmic defaults. We provide ongoing physician access for adjustments, not just initial scripts. Comprehensive male optimization, not transactional prescribing.
We'll review your health profile, lifestyle patterns, and performance goals—then design a personalized approach using the medication or combination that serves your actual life.