Vitamin D3 & Weight Loss: Metabolism, GLP-1 Support & More
Key Takeaways
Low vitamin D is extremely common in people with obesity and is linked to worse metabolic markers and harder weight loss outcomes.
D3 doesn't magically burn fat. But optimizing it improves insulin sensitivity, muscle function, mood, and bone health — all of which matter enormously during a cut or GLP-1 protocol.
For people losing weight quickly on GLP-1 medications, high-dose D3 paired with K2 helps protect bone density and training capacity during a period of rapid body composition change.
Building Blocks provides D3 + K2 as part of a micronutrient safety net designed to work alongside structured training and medically supervised weight loss.
Why Vitamin D Keeps Coming Up in Weight-Loss Conversations
If you've spent any time researching weight loss, you've probably seen vitamin D mentioned alongside metabolism, fat burning, and body composition. The connection is real — but it's not what most clickbait articles suggest.
Here's what the data actually shows: people with obesity are significantly more likely to have low vitamin D levels. Observational studies have consistently found that lower D3 status correlates with higher body fat percentage, more insulin resistance, and poorer outcomes during weight loss interventions. And multiple studies have found that D3 supplementation during caloric restriction is associated with better preservation of metabolic health markers.
What the data does not show is that vitamin D burns fat. D3 isn't a thermogenic. It doesn't accelerate lipolysis. It doesn't replace a caloric deficit, adequate protein, or the structured training that drives real body composition change.
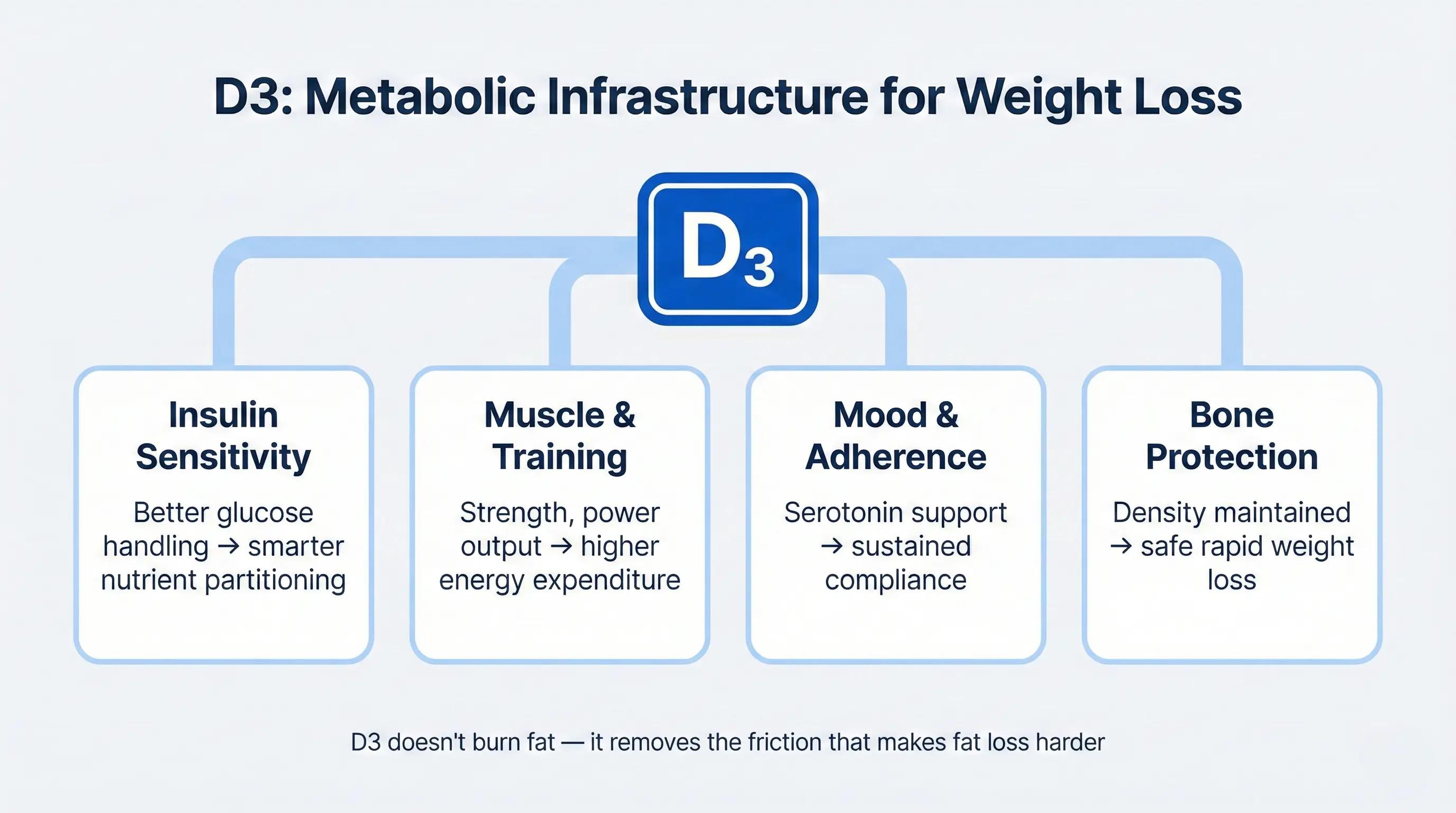
The more accurate frame is this: vitamin D3 is metabolic infrastructure. When it's low, your body operates at a disadvantage — insulin signaling is impaired, muscle function is compromised, mood and energy suffer, and bone integrity is at risk. Optimizing D3 doesn't cause weight loss. It removes biological friction that makes weight loss harder and more costly to your body. For a full overview of what D3 and K2 do together, see our vitamin D3 & K2 benefits guide.
How Vitamin D Affects Metabolism and Body Composition
Insulin sensitivity and glucose handling
Vitamin D receptors are expressed in pancreatic beta cells (which produce insulin) and in insulin-responsive tissues like muscle and adipose tissue. Research suggests that adequate D3 supports healthy insulin signaling — meaning your body handles glucose more efficiently and partitions nutrients more effectively between muscle and fat storage.
During a caloric deficit, this matters. Better insulin sensitivity means the calories you do eat are more likely to fuel muscle maintenance and recovery rather than being shuttled toward fat storage. It's not a dramatic effect on its own, but in the context of a well-structured cut or GLP-1 protocol, it's one of several metabolic advantages that compound over time.
Muscle strength, power, and activity levels
D3 directly influences muscle fiber function and neuromuscular coordination. People with low vitamin D commonly report feeling weaker, more fatigued during exercise, and less motivated to train — all of which indirectly slow weight loss by reducing total energy expenditure and making resistance training less productive.
Correcting a D3 deficit can improve strength output, power production, and the general sense of physical capability that keeps you consistent in the gym. During a weight loss phase, when the goal is to lose fat while preserving as much lean mass as possible, that training capacity is one of the most valuable assets you have. Anything that undermines it — including a preventable nutrient deficiency — is working against you.
Appetite, mood, and adherence
This is the layer most people overlook. D3 influences serotonin synthesis and has been associated with mood regulation in multiple studies. Low D3 during a caloric deficit — which is already a period of physiological and psychological stress — can amplify irritability, low motivation, and the fatigue that makes dietary adherence feel impossible.
No one sticks to a nutrition plan when they feel terrible. Optimizing D3 won't eliminate the discomfort of a deficit, but it can remove one biochemical contributor to the mood and energy crashes that derail compliance. When the margin between success and failure is consistency over months, even modest improvements in how you feel day-to-day add up.
Vitamin D, Obesity, and GLP-1 Therapy
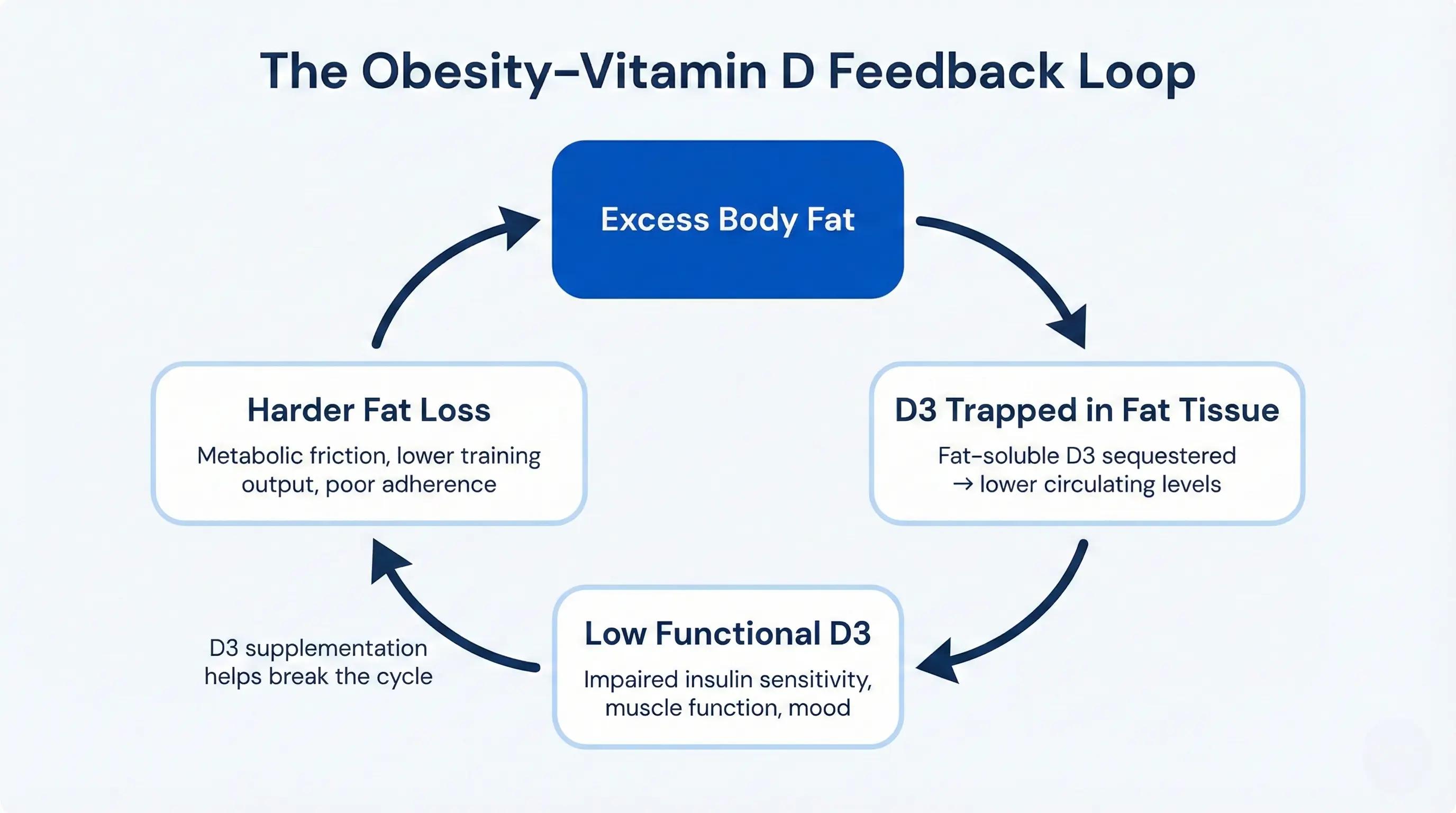
The relationship between vitamin D and body fat runs in both directions. Low D3 is associated with higher body fat, and higher body fat actively lowers circulating D3 levels. Vitamin D is fat-soluble, and excess adipose tissue sequesters it — essentially trapping it where it can't be used. This creates a feedback loop: the more body fat you carry, the lower your functional D3 tends to be, and the lower your D3, the harder certain aspects of metabolic health and weight loss become.
For people on a GLP-1 weight loss protocol, there are additional considerations that make D3 optimization especially important.
First, appetite suppression means lower total food intake, which means fewer micronutrients coming in overall. Fat-soluble vitamins like D3 are particularly vulnerable because their absorption depends on dietary fat, which many people on GLP-1s are also eating less of. Second, rapid weight loss — even healthy, medically supervised weight loss — puts stress on bone density. As fat tissue is lost quickly, the mechanical loading on your skeleton changes, and without adequate calcium, D3, and K2, bone mineral density can decline faster than it should.
This is where the combination of D3 and K2 earns its keep. D3 ensures you're absorbing enough calcium and maintaining the hormonal signaling that supports bone. K2 directs that calcium into bone matrix rather than allowing it to accumulate in arterial walls. Together, they function as a structural safety net during a period when your body is changing rapidly and the risk of collateral damage to bone and muscle is real.
Think of it this way: GLP-1 medications are doing the heavy lifting on fat loss. D3 + K2 help make sure you don't lose the things you want to keep in the process.
What Vitamin D3 Can and Can't Do for Weight Loss
Since the question "does vitamin D help with weight loss?" deserves a direct answer, here it is.
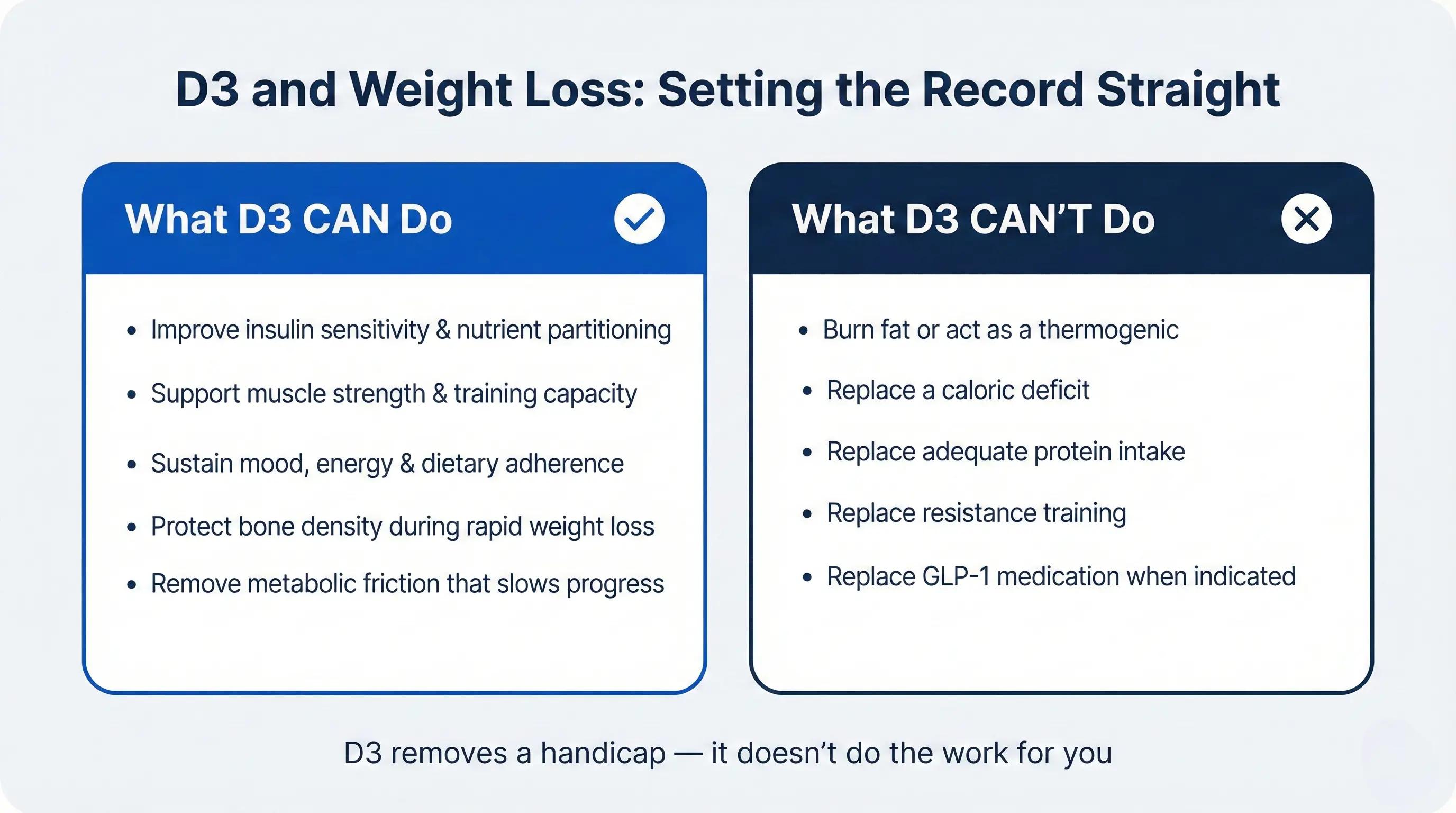
D3 can improve the metabolic conditions under which weight loss happens. It supports insulin sensitivity and glucose handling, which influence nutrient partitioning during a deficit. It supports muscle strength and training capacity, which protect lean mass and drive energy expenditure. It supports mood and energy, which sustain the dietary and exercise adherence that make long-term fat loss possible. And it supports bone health, which prevents one of the most common forms of collateral damage during aggressive weight loss.
D3 cannot replace a caloric deficit. It cannot replace adequate protein intake. It cannot replace resistance training. It cannot replace a GLP-1 medication when one is clinically indicated. And it cannot, by itself, cause your body to burn more fat.
The distinction matters because it's the difference between treating D3 as a responsible part of a weight loss strategy — which it is — and treating it as a shortcut — which it absolutely isn't. Optimizing D3 removes a handicap. It doesn't do the work for you.
How to Use D3 Safely During a Cut or GLP-1 Program
If you're entering a weight loss phase — whether through caloric restriction, a GLP-1 protocol, or both — checking your vitamin D status early is one of the simplest and highest-return moves available. A 25-hydroxyvitamin D blood test tells you exactly where you stand, and it's inexpensive and widely available.
For ongoing supplementation, daily consistency with D3 and K2 is far more effective than sporadic megadoses. Fat-soluble vitamins need to be taken regularly to maintain stable tissue levels, and D3 specifically responds better to steady daily intake than to weekly or monthly boluses.
Always take D3 with a meal that includes some dietary fat — absorption increases substantially when paired with food compared to taking it on an empty stomach. If you're on a GLP-1 and your meals are smaller, even a small amount of fat (eggs, nuts, olive oil, avocado) is enough to support absorption.
If you're taking high-dose D3, periodic lab monitoring of 25-OH D and calcium is the responsible approach — especially during a period of active weight loss when your body composition and nutrient dynamics are changing. And anyone with kidney disease, hyperparathyroidism, or calcium metabolism disorders should work closely with their clinician before starting or adjusting D3 supplementation.
This is why Building Blocks pairs high-dose D3 with K2 (as MK-4) as a standard part of the formulation — so you're not asking your body to change on an empty micronutrient tank. The dose, the pairing, and the lab monitoring that Maximus builds around it are all designed to make aggressive optimization safer and more effective.
Stacking D3 with Other High-Leverage Weight-Loss Strategies
D3 is one essential piece. Here's where it fits within the larger system.
Resistance training combined with a high-protein diet is the single most important strategy for preserving lean mass during weight loss. If you're on a GLP-1 and not training, you're losing muscle along with fat — and that changes your metabolic trajectory in ways that are hard to reverse later.
Magnesium supports sleep quality, stress regulation, and glucose metabolism — all of which interact directly with fat loss outcomes. Vitamin B12 supports the energy production and red blood cell function that keep you performing in the gym rather than dragging through sessions. And for men whose testosterone levels are suboptimal, addressing that hormonal variable can meaningfully improve body composition, motivation, and training response in ways that no micronutrient alone will replicate.
The common thread: none of these work in isolation, and none of them replace the fundamentals (caloric deficit, protein, training, sleep). But each one — D3 included — removes a potential bottleneck that can slow your progress or increase the collateral cost of the weight you're losing.
D3 Won't Do the Work for You — But It Makes the Work Count
Optimizing D3 won't replace a caloric deficit or a GLP-1 medication. What it does is protect the things you don't want to lose while you're losing the thing you do — muscle, bone, mood, and the metabolic health that determines whether your results last.
For anyone on a GLP-1 protocol or pursuing aggressive fat loss, the cost of ignoring D3 is real: compromised bone density, impaired training capacity, worse mood and adherence. The cost of addressing it is a daily supplement and a periodic lab check. That math is simple. Building Blocks includes high-dose D3 paired with K2 precisely because the goal isn't just weight on the scale — it's a body that's stronger and healthier on the other side of the cut.
Vitamin D3 & Weight Loss — FAQs
Will taking vitamin D3 alone make me lose weight?
No. Vitamin D3 is not a fat burner and will not cause weight loss on its own. What it does is support the metabolic conditions — insulin sensitivity, muscle function, mood, bone health — that make weight loss more effective and sustainable when combined with a caloric deficit, adequate protein, resistance training, and (when appropriate) GLP-1 therapy. Think of it as removing a handicap, not as the engine.
What vitamin D level should I aim for when trying to lose weight?
Work with your clinician to interpret your 25-hydroxyvitamin D levels in context. Most performance-oriented providers target levels well above the conventional "sufficient" threshold, aiming for an optimal range that supports metabolic and hormonal health rather than simply avoiding clinical deficiency. Your starting level, body composition, and supplementation dose all factor into what target makes sense for you.
Do GLP-1 medications lower vitamin D levels?
Not directly through a pharmacological mechanism, but indirectly through reduced food intake. GLP-1 medications suppress appetite, which means you're consuming less of the dietary fat needed for fat-soluble vitamin absorption and fewer overall nutrients. Combined with the rapid body composition changes that GLP-1s produce, this makes monitoring and supplementing D3 especially important throughout the protocol.
Is there a best time to take D3 during a cut?
With a meal containing dietary fat — that's the most important variable. Morning or midday tends to be most practical and avoids the theoretical (though not strongly evidenced) concern about evening D3 interfering with sleep. Consistency matters far more than precise timing. If you're taking it as part of a daily multivitamin like Building Blocks, morning with your first meal is the simplest approach.